Dropping it in the mail: Best practices detailed for mail-in colon cancer screenings
DALLAS – Sept. 8, 2020 – A program that asks patients to mail in stool samples to screen for colon cancer is an effective way to expand screenings to underserved and underinsured communities and offers an alternative to in-person testing during the pandemic, according to a study conducted by UT Southwestern.
In an article published recently in CA: A Cancer Journal for Clinicians, UT Southwestern physicians identified nine best practices for effective mail-in screening campaigns, which can take the place of invasive, unpopular colonoscopies.
While doctors say that mail-in stool samples bring new meaning to the phrase “dropping something in the mail,” they also note that this program is a way to continue cancer screenings while keeping people out of clinics and hospitals during the COVID-19 pandemic.
It’s also cost-effective and just as capable of detecting cancer as a colonoscopy.

“This project is succeeding in making cancer screenings less invasive and more widely available. Serendipitously, it now has the added benefit of being yet another way to keep people out of hospitals and clinics during pandemic shutdowns,” says Amit Singal, M.D., an author of the study, professor of internal medicine and population and data sciences, medical director of the Liver Tumor Program, and clinical chief of hepatology at UT Southwestern.
More than 53,200 Americans are expected to die of colon cancer in the United States in 2020, according to the National Cancer Institute.
The best practices identified in the article are:
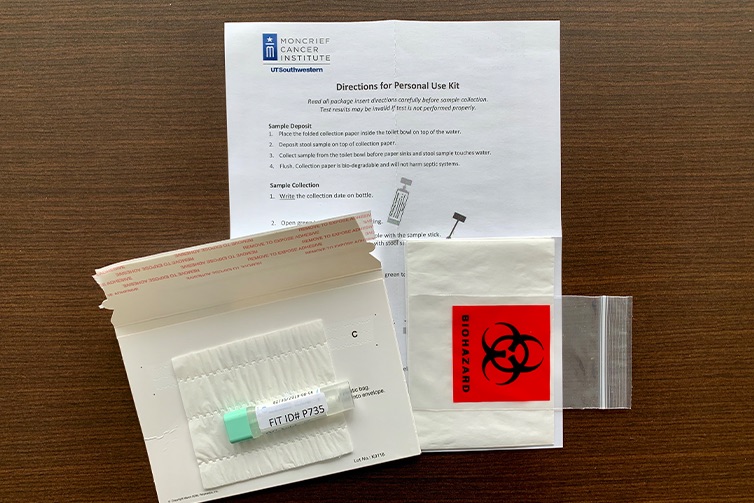
- Reach out to recipients with texts, telephone calls, and printed mailings before sending them the fecal immunochemical testing kit, or “FIT kit.”
- Ensure the invitation letters are brief and easy to read.
- Keep instructions simple and address challenges that may lead to failed laboratory processing.
- Send reminders to recipients who do not return their tests.
- Use data infrastructure to track each step of the outreach process.
- Have protocols and procedures, such as patient navigation, in place to promote a colonoscopy if a FIT test shows abnormal results.
- Use high-quality FIT tests.
- Ensure the program has a champion, organizational support, and sufficient funding.
- Push for wide implementation to increase the program’s efficacy and efficiency.

The best practices were learned from mailed FIT campaigns throughout the United States, including one that reached more than 108,000 people in 25 North Texas counties including Tarrant County. Another campaign reached more than 15,000 persons at Parkland Health & Hospital System, the Dallas County safety-net health system. Nearly a third of the FIT kits were returned by recipients, and approximately 5 percent of them returned positive.

“What the test enables you to do is say you can do this in the privacy of your own home. A lot of people prefer that,” says Keith Argenbright, M.D., director of UT Southwestern’s Moncrief Cancer Institute in Fort Worth and a professor in the Harold C. Simmons Comprehensive Cancer Center.
Returned stool samples were tested for a blood antigen associated with colon cancer, and patients who tested positive were told they needed to schedule a diagnostic colonoscopy. Follow-up with patients from Dallas County was performed by UT Southwestern staff, and follow-up with patients from other counties was handled by staff from the Moncrief Cancer Institute, which is part of the Simmons Cancer Center.
Argenbright said oncologists nationwide fear cancer deaths will spike several years from now because many cancers will go undetected as people put off colonoscopies and other screenings during the pandemic.
“We think this is an extremely timely solution to the current pandemic,” he says. “Even though screening efforts restarted, patients are still afraid to come in.”
Additional study authors are Samir Gupta, Gloria D. Coronado, Alison T. Brenner, Sheila F. Castañeda, Jason A. Dominitz, Beverly Green, Rachel B. Issaka, Theodore R. Levin, Daniel S. Reuland, Lisa C. Richardson, Douglas J. Robertson, Michael Pignone.
The publication was supported by a grant or cooperative agreement (NU38OT000286-01-01) funded by the Centers for Disease Control and Prevention. Singal receives funding from the Cancer Prevention and Research Institute of Texas (PP160075). Argenbright and Singal receive funding from CPRIT, (PP160075 and PP200009).
Singal reports personal fees from Exact Sciences outside the submitted work. No other disclosures were made.
<
About UT Southwestern Medical Center
UT Southwestern, one of the nation’s premier academic medical centers, integrates pioneering biomedical research with exceptional clinical care and education. The institution’s faculty members have received six Nobel Prizes and include 24 members of the National Academy of Sciences, 25 members of the National Academy of Medicine, and 13 Howard Hughes Medical Institute Investigators. The full-time faculty of more than 3,300 is responsible for groundbreaking medical advances and is committed to translating science-driven research quickly to new clinical treatments. UT Southwestern physicians in more than 80 specialties care for more than 143,000 hospitalized patients, attend to more than 470,000 emergency room cases, and oversee nearly 5.3 million outpatient visits a year.