High-Resolution Pharyngeal Manometry: A New Tool for Dysphagia Assessment, Biofeedback, and Progress Monitoring
Melanie Turner Tice, M.S., CCC-SLP
April 16, 2026
When modified barium swallow studies and fiber-optic endoscopic evaluations of swallowing are unrevealing, high-resolution pharyngeal manometry may provide a supplemental diagnostic tool to identify physiologic deficits in challenging cases of dysphagia.
For example, pharyngeal contractile strength, bolus pressurization patterns, and UES relaxation pressures can clarify whether pharyngeal weakness or UES dysfunction primarily contributes to an impairment in swallowing in individuals who demonstrate both types of deficits.
Another new diagnostic category made possible with the manometry is that of pharyngeal hypercontractility. The 2025 Leuven Consensus published by the International High Resolution Pharyngeal Manometry Working Group includes criteria for diagnosing abnormally high pharyngeal pressures, which – though less often discussed – can also be maladaptive. This type of dysfunction may not be readily identified using standard imaging evaluations, but its diagnosis is critical; swallow strengthening exercises may be contraindicated for this type of patient if they perpetuate maladaptive hypercontractility.
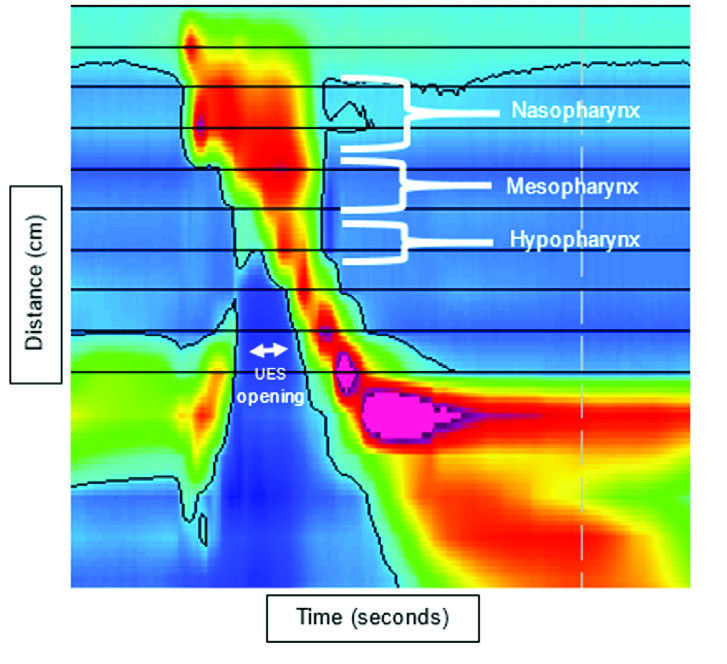
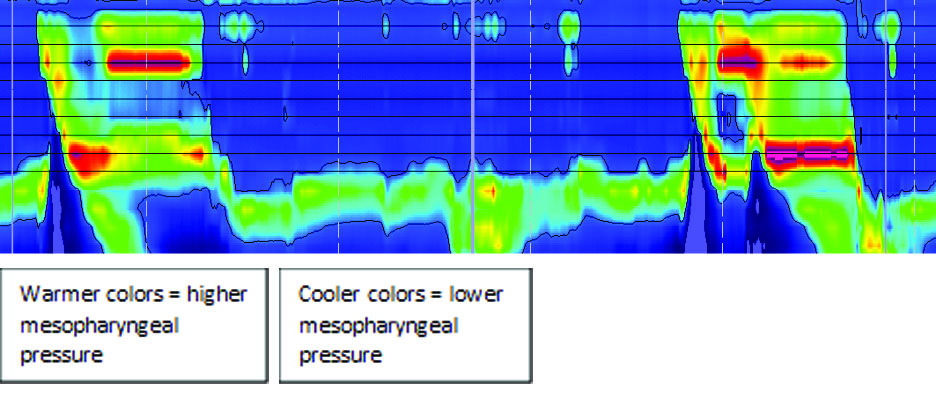
Therapeutically, the manometry is useful for biofeedback training. The colorful depiction of swallowing pressures can help individuals learn and practice swallow exercises. Specifically, patients can use this visual input to monitor the effectiveness of their swallowing and refine their approach to improve outcomes. For example: Notice how, when this individual first attempted the Mendelsohn maneuver (an exercise designed to sustain the mesopharyngeal squeeze after the swallow), the manometric image shows warmer colors in the nasopharynx and cooler colors in the mesopharynx during the time when the individual is attempting to sustain the laryngeal hold.
With visual biofeedback and cues to increase the warmth of color in the mesopharyngeal area, the individual attempted the exercise a second time with reduced warmth in the nasopharyngeal region and increased warmth in the mesopharyngeal region, thereby completing the exercise in the target range.
A third, important application of high-resolution pharyngeal manometry is progress monitoring. The pressurized catheter used for this evaluation is sensitive to subtle changes in physiologic pressures, thereby quantifying an individual's response to intervention even before clinical signs of improvement become apparent. This type of feedback provides valuable insight to clinicians, who then may consider pivoting to a new therapeutic method rather than continuing an approach long enough to realize clinical changes are not occurring.
With such promising applications, we look forward to continuing to implement this tool with many patients to come, improving effectiveness and efficiency of dysphagia diagnosis and treatment.