Extended Cricotracheal Resection With Cartilage Grafting for Concurrent Glottic and Subglottic Stenosis
Kevin Liang, M.D.
Director, UTSW Complex Airway Program
April 16, 2026
UT Southwestern established a Complex Airway Program, which includes a multidisciplinary team of otolaryngologists, thoracic surgeons, interventional pulmonologists, and rheumatologists. We are excited to provide innovative and advanced interventions for all types of airway disease.
This includes definitive surgery for patients with concurrent posterior glottic stenosis (PGS) and subglottic stenosis (SGS). In this population, traditional interventions to address either PGS or SGS alone are insufficient for tracheostomy decannulation without addressing the other level of stenosis.
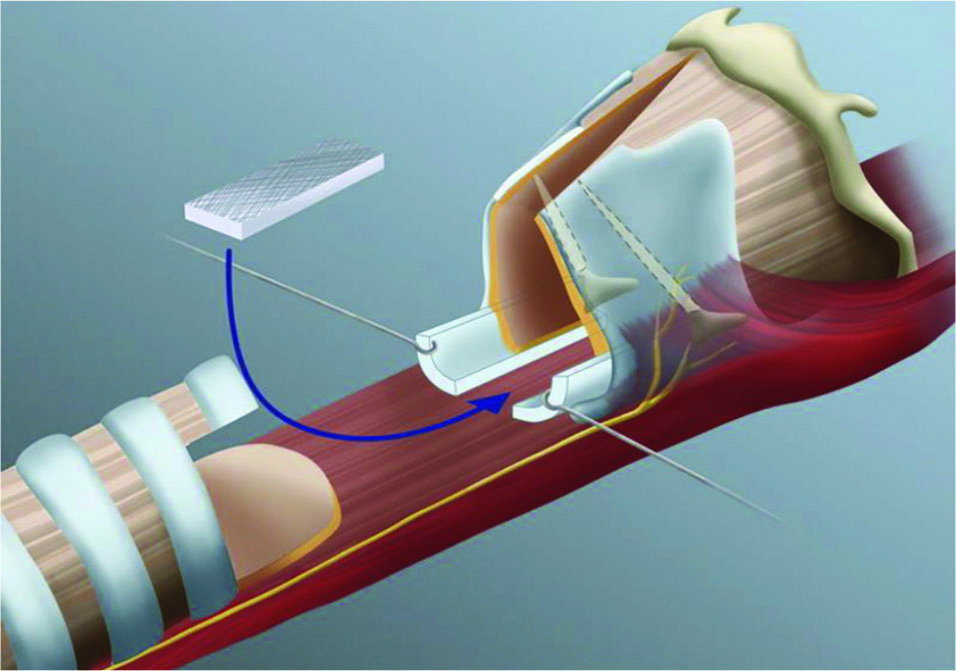
The extended cricotracheal resection (eCTR) combines a traditional CTR (resection of the anterior cricoid arch and proximal trachea) with laryngofissure, posterior cricoid split, and cartilage graft augmentation of the posterior glottis. The laryngofissure is executed in the midline to avoid injury to the true vocal folds. The fibrotic posterior glottic mucosa is resected, and the posterior plate of the cricoid is split in the midline. A cartilage graft (either autologous or cadaveric) is then sutured in place between the cut edges of the posterior cricoid plate. A posterior trachealis flap is fashioned from the distal tracheal segment to cover the cartilage graft and create a fully mucosalized airway. The laryngofissure is then closed, paying special attention to realigning the glottic anterior commissure. The thyrotracheal anastomosis is closed in a running fashion. A new tracheotomy is created multiple rings below the anastomosis. A suprastomal stent is placed for six weeks to allow the cartilage graft to integrate. Additional bronchoscopies may be needed to address any granulation tissue prior to safe decannulation.
Case Example
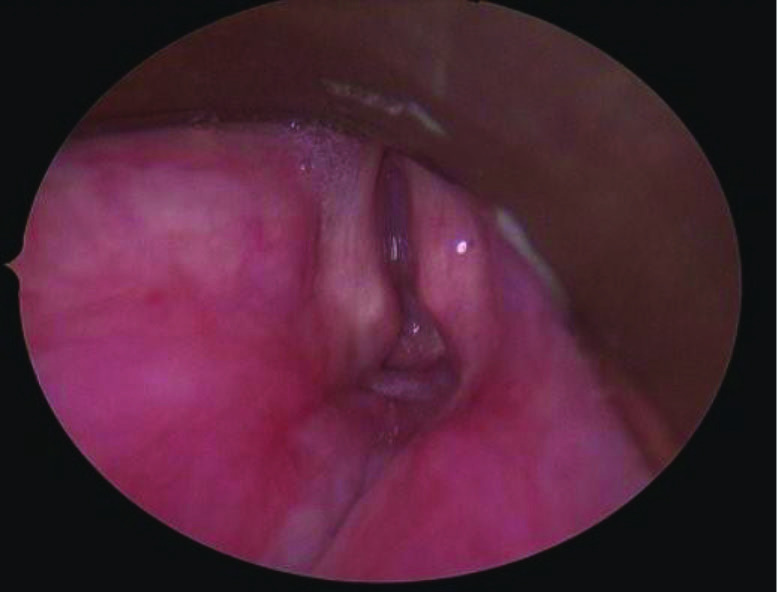
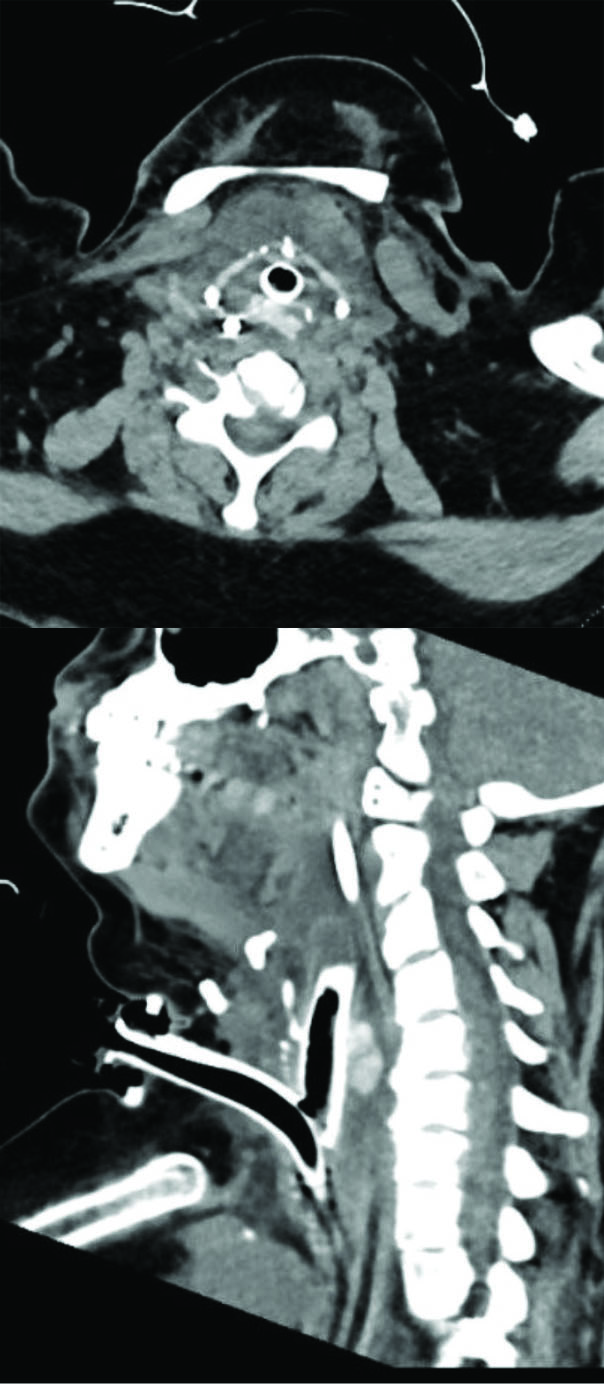
This is a female in her 40s who is a patient of Dr. Liang's. She had a prolonged intubation and developed severe posterior glottic stenosis along with Grade 4 100% subglottic stenosis.
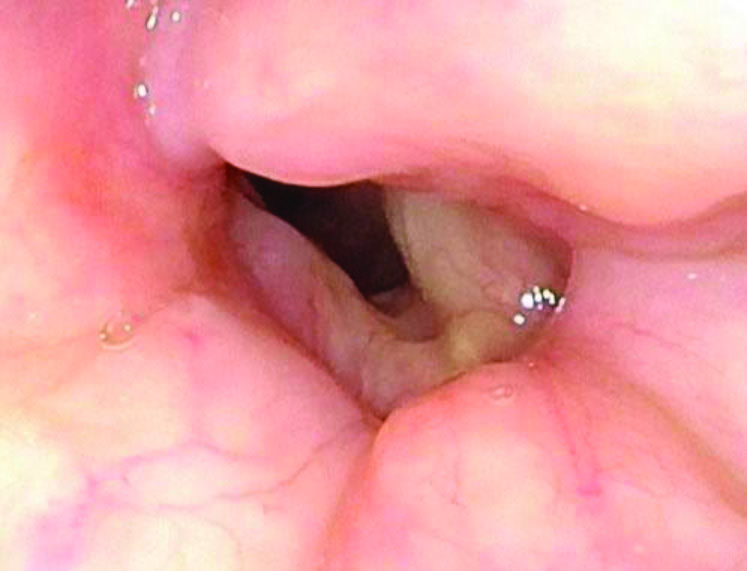
This patient underwent extended cricotracheal resection with posterior cricoid cartilage grafting. She has been decannulated for over six months and is breathing very well. Her voice is breathy, as anticipated, but it is fully understandable. Also, the patient is very happy to be rid of the tracheostomy.
Monnier, Philippe. “Partial Cricotracheal Resection and Extended Cricotracheal Resection for Pediatric Laryngotracheal Stenosis.” Thoracic Surgery Clinics. Vol. 28,2 (2018): 177-187. doi:10.1016/j. thorsurg.2018.01.012