

Teaming with insight
{kind=link}

When Dr. Jonathan Cohen arrived in Dr. Helen Hobbs’ lab to learn genetics, the pairing was unexpected – neither had chosen the other.
“He was a postdoc in my laboratory with no background in genetics, but a deep understanding of lipoprotein physiology,” Dr. Hobbs says. “He was a quick learner, avid reader, and good experimentalist.”
A decade later, the two forged a partnership widely credited with laying the scientific foundation for a new class of cholesterol-lowering drugs – and there’s more to the story.
As the drugs that grew out of their research sailed through clinical trials, the two scientists launched a new investigation. Working on the genetics of the emerging threat of nonalcoholic fatty liver disease (NAFLD), they identified the first gene for the condition.
The story of this pair is also the tale of a unique place: UT Southwestern.
Their partnership overcame what many would consider impediments, including differences in background and temperament.

Boston native Dr. Hobbs graduated from Stanford University, completed medical school at Case Western Reserve University, and served an internship at Columbia-Presbyterian Medical Center before arriving at UT Southwestern during the 1980 heat wave for her residency.
“It was 114 degrees. Terrible,” she says with a laugh, adding that she was focused on throwing herself into her medical training.
On an August day nine years later, Dr. Cohen arrived at UTSW, with a fresh Ph.D. from the University of Cape Town in South Africa. He began working as a postdoctoral researcher in UT Southwestern’s Center for Human Nutrition under its then-Director Dr. Scott Grundy, Professor of Internal Medicine, whose work on dietary fats and cholesterol metabolism was already legend.
Dr. Cohen’s first impression of Texas?
“Hot,” he says. “As I walked off the plane onto the jet bridge, I thought they’d parked the plane in such a way that we were standing in the jet exhaust. I soon found that wherever you went, the temperature stayed the same.”
Early in his postdoc work in metabolism, Dr. Cohen realized he needed to learn genetics. He went to ask his mentor, Dr. Grundy, for permission to spend a few weeks in another laboratory on campus learning techniques from others at his level. Instead of merely supporting the idea, Dr. Grundy was all in. He went to Dr. Hobbs – then an Assistant Professor of Internal Medicine and Molecular Genetics as well as Chief of the Division of Medical Genetics at the UT Southwestern Medical School – to suggest she take over Dr. Cohen’s training.
“Dr. Grundy’s generosity toward me was remarkable. I have never heard of anything like it,” Dr. Cohen says. As a fellow in the Center for Human Nutrition, Dr. Cohen was considered one of the Center’s most promising postdoctoral researchers.
Characteristically cool, Dr. Cohen’s most emotional response – expressed in strictly scientific terms – comes when asked to describe his first impression of Dr. Hobbs.
“She just radiated energy,” he says.
After he finished his fellowship, Dr. Cohen became a faculty member in the Center for Human Nutrition. The two studied different aspects of cholesterol genetics and kept in touch.
“I was focusing on the genetics of plasma low-density lipoprotein (LDL) cholesterol and lipoprotein (a) (Lp(a)) levels, while he worked on the genetics of plasma high-density lipoprotein (HDL) cholesterol. We continued to talk about our science, sharing a deep interest in human genetics,” Dr. Hobbs says.
By 1999, Dr. Cohen had attained tenure and the two came together for three intense weeks while writing the population science section of the massive Dallas Heart Study (DHS), the largest study of its kind in North Texas. Dr. Cohen is now a Professor in the Center for Human Nutrition, in the Eugene McDermott Center for Human Growth and Development, and of Internal Medicine, as well as holder of the C. Vincent Prothro Distinguished Chair in Human Nutrition Research.
“The DHS is typical Helen, it encapsulates her,” Dr. Cohen recalls. “The way she set out to do the study by asking, ‘What is the best possible study we could do assuming there were no logistical or financial limitations? What would be the ideal study?’”
Designing a massive study
They created an epidemiological study structured as if it were bench science in which every step and measurement had complete quality control and every detail was addressed with utmost care.
“That was a terrifically enjoyable process as we conceived of the best experiments we could envision using a human population. As luck would have it, the grant was funded and we decided to join our laboratories,” said Dr. Hobbs, Director of the Eugene McDermott Center for Human Growth and Development and a Howard Hughes Medical Institute Investigator since 2002 as well as a Professor of Internal Medicine and Molecular Genetics at UTSW. Dr. Hobbs also became Director of the Dallas Heart Study when its original leader left the University.
One afternoon, Drs. Hobbs and Cohen were discussing how to proceed with their now-funded project and all of the additional research programs to which they were committed.
“I proposed that the most practical thing would be to fuse our efforts. I think there was a sense that this was inevitable,” Dr. Cohen says.
“We can openly and honestly criticize each other’s thoughts, ideas, and interpretations of data. This approach allows us to think more expansively without always having to self-edit our thoughts.”
Although she doesn’t recall the moment, Dr. Hobbs remembers the feeling of inevitability.
“It seemed like a natural progression after sitting in the same room together writing the Dallas Heart Study grant. It was clear to me from that experience that we were better together than apart,” she explains. In 2000, they created the Hobbs-Cohen lab.
“I am more extroverted, and he is more of an introvert. I am very focused in my interests and in where I want to take our science. He is interested in everything. He is more of a scholar in the academic tradition than I am. Jonathan is an exceedingly calm, measured, and patient man. I am not such a woman,” says the gregarious Dr. Hobbs.
“Helen is very intuitive and arrives at things very quickly. She can see end goals when they are still murky for me,” Dr. Cohen says. “I’m analytical, I like to frame my thoughts in a step-by-step process. These are really generalizations. There are many instances where Helen is systematic and will find holes in my thought process. It’s not all or none, it’s a tendency.
“Helen’s design and running of the DHS is as logically consistent as they come: her saying, ‘What would the best study be and how will we get there?’” he adds.
Dallas Heart Study findings
In 2006, the Hobbs-Cohen lab reported that mutations inactivating PCSK9 conferred protection from heart disease. They also identified an African-American mother and aerobics instructor who had two rare genetic mutations in PCSK9 that resulted in strikingly low blood levels of artery-clogging LDL cholesterol. They noted that exhaustive medical testing in their lab at the McDermott Center had turned up no ill effects from living without PCSK9 (proprotein convertase subtilisin-like kexin type 9).
Their reports are widely credited with providing the scientific basis for what became a race among drug companies to develop PCSK9 inhibitors as cholesterol-lowering drugs. The drugs are targeted to patients unable to tolerate statins or those whose LDL blood levels remain above goal despite other treatments.
It also marked a case of lightning striking twice. Dr. Hobbs was learning bench science in the joint laboratory of Dr. Michael S. Brown and Dr. Joseph L. Goldstein when the two shared the 1985 Nobel Prize in Physiology or Medicine for their work on the LDL receptor, widely hailed as providing the scientific underpinning for development of the statin class of cholesterol-lowering drugs.
The Hobbs-Cohen work on the liver disease NAFLD dates back to the first phase of the DHS. “We were interested in liver fat content from the start,” Dr. Cohen says. It is well-established that some individuals who refrain from consuming alcohol develop a type of liver disease that is usually seen in alcoholics.
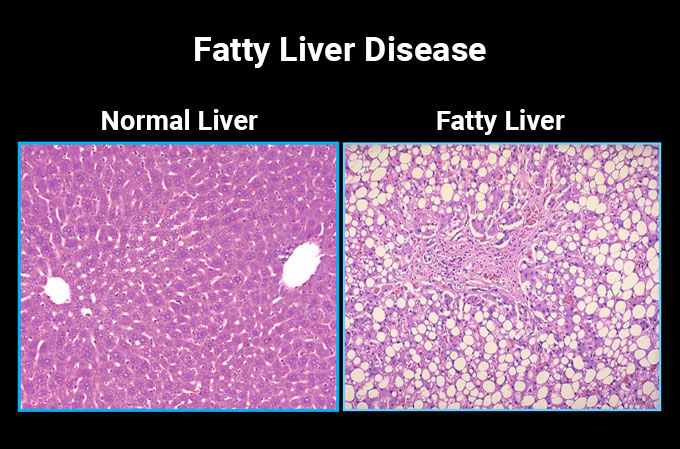
NAFLD represents a continuum that starts with the buildup of fat in lipid droplets in the interior (the cytoplasm) of liver cells – a condition called steatosis (fat in the liver). About 25 percent of people who get steatosis develop associated inflammation and fibrosis. A subset of those individuals will further develop cirrhosis and some of them will develop liver cancer, Dr. Hobbs says.
During the writing of the DHS population science section, the two predicted the technology for genetics research would advance quickly, allowing for the identification of DNA sequence variations that contribute to disease.
The rate-limiting step in applying any new genetics technology would be a population of individuals who had been carefully evaluated for health-related parameters. Therefore, when writing the DHS, they proposed to collect high quality data on phenotypes (traits). “Same tests, on the same people, administered by the same staff, at the same place – if you could get that, then noise associated with the resulting measurements would be minimized,” Dr. Cohen says.
They decided to measure fat in the liver using magnetic resonance spectroscopy (MRS), making their study the first population science investigation of fatty liver disease employing a highly accurate, quantitative method to measure fat in the liver noninvasively. No one had reported using MRS on that scale, and it was the first such study on a healthy population.
They found a distribution of hepatic fat that ranged from almost none to 30 percent. When they narrowed their focus to DHS participants at or above the 90th percentile for liver fat, the scientists found that African-Americans were underrepresented and Hispanics were overrepresented. The difference appeared independent of body weight or insulin resistance, two major factors known to promote NAFLD.
Pinpointing a genetic variant
The Hobbs-Cohen partnership went to work writing another grant to pay for a genetic screen that was quite expensive at the time. With the new funding, they ran the screen and identified the world’s first sequence variation contributing to the development of NAFLD. A substitution of one amino acid at position 148 of the PNPLA3 gene remains the most important sequence variation contributing to the condition, they say.
“I suspect partnerships are idiosyncratic to the people involved. I think ours works because we are very different. If we thought the same things in the same way, we wouldn’t need each other.”
The researchers found that while the gene variant is uncommon in African-Americans, 49 percent of Mexican-Americans have one variant in their two copies of PNPLA3 and 25 percent have two variants. Yet even in those with two copies of the variant gene, NAFLD doesn’t show up unless they are overweight. “Genotype isn’t the only thing. You have to have an increase in body weight,” Dr. Hobbs says. In one study, no one in the normal weight (body mass index below 25 kg/m2) group had NAFLD even if they had two copies of the gene variant while almost all of those considered obese (body mass index equal or greater than 30 kg/m2) had NAFLD, Dr. Hobbs says.
Sorting out the mechanism underlying these findings is taking many conversations, and they tend to spend the most time discussing experiments conducted in the Hobbs-Cohen laboratory with unexpected results, Dr. Cohen says.
“We balance each other well on every level: in our personalities, our scientific orientations, and in our strengths. For example, I am better at making figures for papers and presentations, whereas he is better at writing,” says Dr. Hobbs, who holds the Eugene McDermott Distinguished Chair for the Study of Human Growth and Development, the Philip O’Bryan Montgomery, Jr., M.D. Distinguished Chair in Developmental Biology, and the 1995 Dallas Heart Ball Chair in Cardiology Research.
“I suspect partnerships are idiosyncratic to the people involved,” Dr. Cohen says. “I think ours works because we are very different. If we thought the same things in the same way, we wouldn’t need each other.”
“We can openly and honestly criticize each other’s thoughts, ideas, and interpretations of data. This approach allows us to think more expansively without always having to self-edit our thoughts. Plus, working together makes the whole process more fun. We both love science, talking about science, working out problems, and running a lab,” Dr. Hobbs says.
Dr. Goldstein, a Regental Professor, is Chair of Molecular Genetics and a Professor of Molecular Genetics and Internal Medicine. He holds the Julie and Louis A. Beecherl, Jr. Distinguished Chair in Biomedical Research and the Paul J. Thomas Chair in Medicine.
Dr. Brown, a Regental Professor, is Director of the Erik Jonsson Center for Research in Molecular Genetics and Human Disease, as well as a Professor of Molecular Genetics and Internal Medicine. He holds The W.A. (Monty) Moncrief Distinguished Chair in Cholesterol and Arteriosclerosis Research and the Paul J. Thomas Chair in Medicine.